
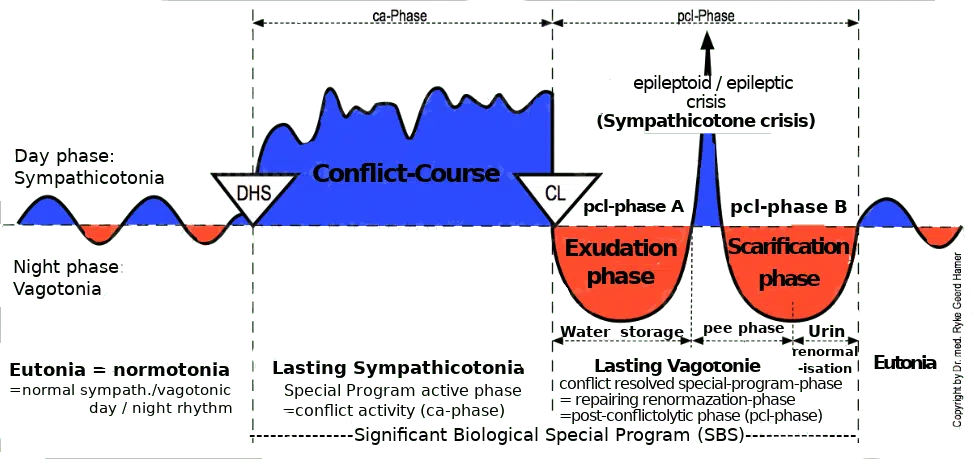
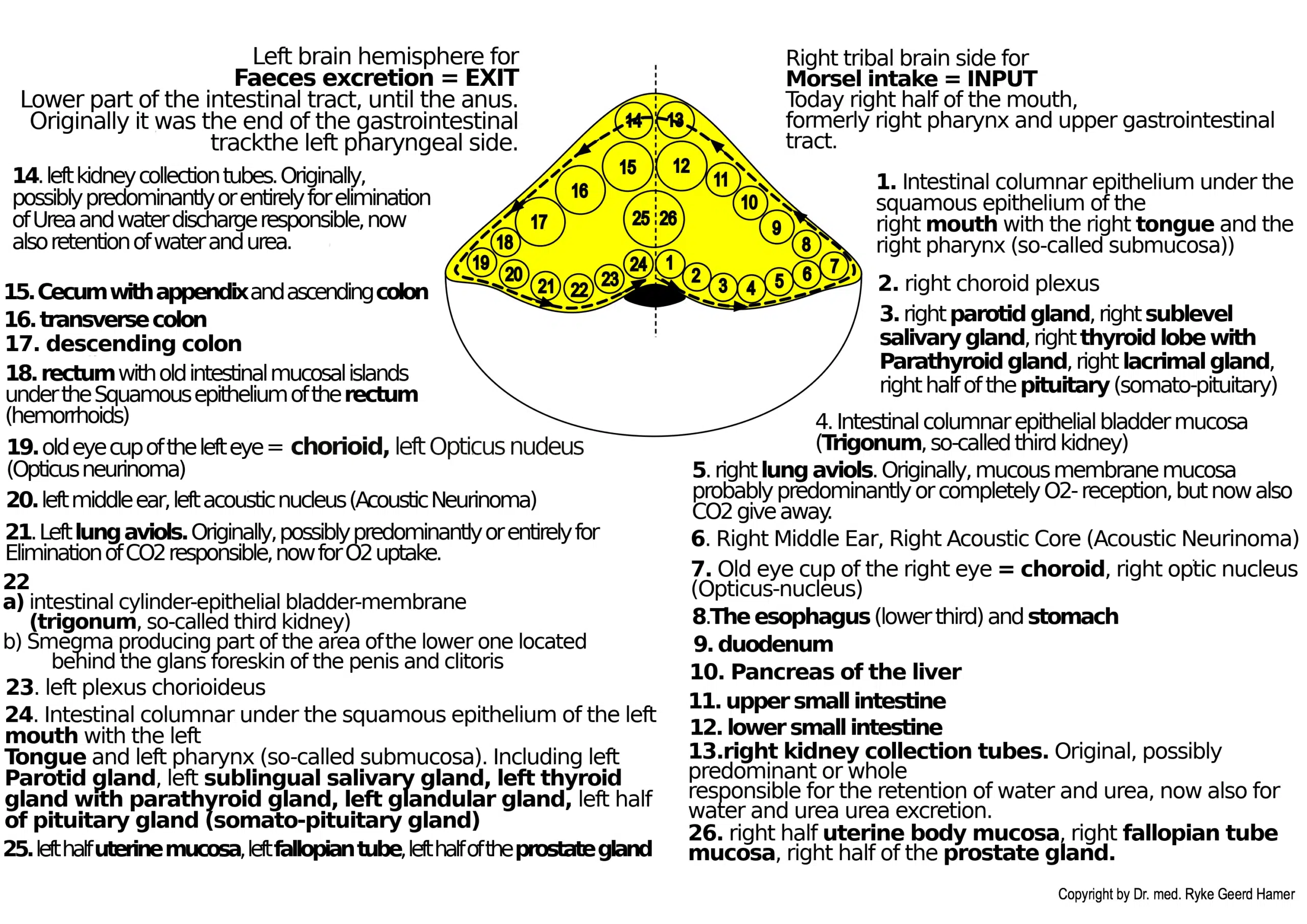
Brainstem = Old Brain = Inner Germ Layer = Endoderm
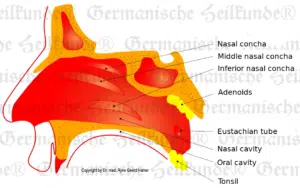
Tonsil Cancer left – Diagnostic Chart
Conflict of not being able to spit out a (fecal) morsel due to lack of secretion.
In the ancient pharyngeal period, saliva was also used to help the feces slide out of the pharynx’s orifice. The excrement was “salivated.” From it still our “spitting out” wants (with the secretion of the salivary glands) and “throwing up” wants, namely the excrement morsel. Mucus and saliva are the same.
Since there is no more gullet but only a “mouth,” the conflict is predominantly “transferred,” understood as spitting out and wanting to vomit out.
Wanting to vomit out, wanting to spit out.
HH in the brainstem left dorsal
Tonsillar hyperplasia = tonsillar hypertrophy = cauliflower-like growing adeno-ca of secretory grade. Enlarged, often “fissured” tonsils when multiple adenocarcinomas with tuberculous caseation had already expired in the pcl-phase.
Fetid tuberculous caseation of tonsillar hyperplasia: purulent tonsillitis, tonsillar abscess caused by fungi (tonsillar mycosis), or fungal bacteria (tonsillar TB).
Centralization
–
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |
You’ll be informed by email when we post new articles and novelties. In every email there is a link to modify or cancel your subscription.



