The trigger of every so-called disease is always a biological conflict, a highly dramatic shock experience called a DHS. In the second of the DHS, a responsible relay center in the brain is marked, a circular shooting target configuration (Hamer Focus), which corresponds with a certain organ. The more extensive this Hamer Focus (HH) is, the more extensive the tumor, necrosis, or change of cells in the organ.
The DHS is the basic building block of the Iron Rule of Cancer (IRC), the basis of a revolutionary understanding of all Germanische Heilkunde®. Most patients know the exact moment of the DHS because it was always dramatic.
In Germanische Heilkunde®, every so-called disease has two phases: the first is cold, and the second is hot if the conflict is solved. However, suppose the conflict cannot be resolved; in this case, the “disease” remains single-phase, i.e., the individual remains in the conflict-active phase, becomes more and more emaciated, and may eventually die of debilitation or cachexia. Up until now, we had always overlooked the complementary part, which made our conventional medicine theories erroneous from the ground up.
1. One type makes cell proliferation in the conflict-active, sympathicotonic phase.
2. The second type makes cell proliferation in the vagotonic healing phase, as in diseases that have formed cell atrophy, i.e., holes, necroses, or ulcers in the conflict-active phase.All tumors formed in the conflict-active phase by cell proliferation have their brain relays located next to each other. They also belong to the same germ layer for developmental reasons and have a special biological meaning. Each of these germ layers belongs to:
– a specific brain part,
– a specific type of conflict content
– a particular histological cell formation
• a very specific germ layer-related microbes.
This basic pattern is valid for all three germ layers and the so-called diseases of the organs deriving from them. All cancerous diseases that make cell multiplication in the conflict-active phase have their relay, from which they are directed, in the brainstem and cerebellum – thus in the old brain.
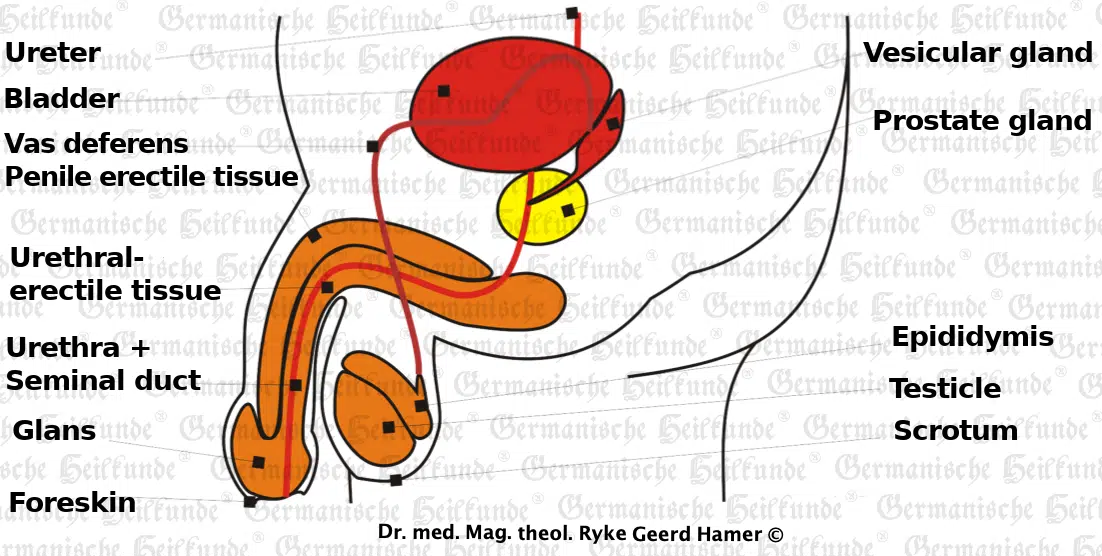
The prostate-Ca belongs to the brainstem organs and, therefore, makes compact tumors of the adeno-cell type in the conflict-active phase. The conflict content is always an ugly, semi-genital conflict, which means that the conflict content’s focus does not revolve around the purely genital area (in the natural or figurative sense). Still, the genital theme occurs as an accompaniment, making this conflict distinctly different from the sexual conflict.
Here are some typical prostate conflict examples:
• A favorite daughter sues her father for alimony or early surrender of her inheritance
• An only daughter has gone off the rails and/or is a drug addict
• A man catches his wife/mistress in flagrante delicto with a younger lover, and repulsive things come to light during a divorce
• A young girlfriend leaves her older man in favor of a younger man …
In the conflict-active phase, a compact tumor of the adeno-cell type grows. As with all tumors of the old-brain controlled organs, the mycobacteria (if any are present) multiply at the same time, although they will perform their actual task only in the conflict-resolved phase.
The stronger the conflict is, the faster the tumor grows. The longer the conflict lasts, the bigger the tumor becomes. Apart from the vegetative parameters, such as insomnia, loss of appetite, weight loss, etc., the patient does not experience any pain or other discomfort. Only in those cases (about 10%) where the prostate-ca happens to press onto the urethra a delayed urine flow can be observed (weaker urine stream).
The prostate-ca does not hurt either in the ca-phase or in the pcl-phase (healing phase). If the conflict is resolved, then everything behaves in precisely the opposite way: the patient sleeps again, eats again, and gains weight again. The mycobacteria, which multiplied during the conflict-active phase, become active and break down the tumor. The urine is foul-smelling, cloudy (tuberculous), and sometimes mixed with some blood. This is nature’s surgery.
The patient sweats at night and is very tired. He has a fever, not infrequently up to 40 °C, but all this is harmless. The patient only has to eat well with lots of proteins. Also, due to the swelling in the healing phase, the urethra can be temporarily compressed. In this case, an indwelling catheter should be inserted for 1-2 months until the tumor is tuberculated and the urine outflow obstruction is gone. After that, everything will be okay again.
Tuberculous prostate healing (possibly with a temporary indwelling catheter) is entirely harmless and also not painful as long as the urine has drainage. Only the so-called “planning” of the prostate through the urethra is dangerous because the patient usually becomes impotent (due to injury to the nerves). However, impotence is not always an outcome of prostate-ca.
Even in the absence of mycobacteria, nothing significant happens now in 90% of cases, except that urine flow may be somewhat slowed by a general swelling of the prostate. But again, renormalization occurs at the end of the decongesting.
In the remaining 10 % of cases where the cell proliferation has pushed into the urethra and is now no longer being cleared due to mycobacteria’s absence, surgery may have to be considered. Taken together, however, this would be only about 5% of the cases in which surgery would have to be considered at all, and only because there was a non-biological course, i.e., no mycobacteria were present at the time of the conflict activity.
We have always regarded microbes as evil enemies or as an army of virulent opponents who want to destroy us, and therefore, we should exterminate them if possible. Now in the ontogenetic-conditional system of tumors and cancer equivalents, we understand microbes to be our very best friends, helpers, quasi-good garbage men, and restorers of our organism. They work relatively well-behaved only when our organism gives them the explicit command from the brain to do so, namely, always precisely at the beginning of the healing phase when the organism switches from permanent sympathicotonia to permanent (healing) vagotonia.
In conventional medicine, the only aim was to eliminate the tumor, or what was considered a tumor. Regardless of whether this tumor had grown in the conflict-active phase or whether it was a healing phase, cell growth was always cut out. It was always assumed that the cancerous tumor must originate from a cell gone wild that had swum through the arterial blood to other organs and created a new cancer there, which they refer to as “metastases.” However, if cancer cells could swim away to distant organs, they would necessarily have to get there through the arterial blood because the venous system and the lymphatic channels lead only to the center, i.e., the heart. No researcher has ever been able to find a cancer cell in arterial blood.
Thus, if a diagnosis is “metastases,” this implies an unproven, even false, hypothesis that any secondary carcinomas found are so-called daughter tumors of the primary carcinoma. The fact that there may be a second or even third carcinoma is not disputed, at least not in principle, but the evaluation of this indisputable fact and its links. After all, how could a prostate-Ca, which makes compact tumors in the conflict-active phase, be able to migrate, for example, into the bones to fabricate cellular atrophy there.
The Germanische Heilkunde® is not a hypothesis medicine. It is based solely on five biological laws of nature and is, in each case, on all three levels – psyche, brain, and organ – and precisely provable and strictly reproducible.
Therefore, based on the recent findings of Germanische Heilkunde®, we have to think carefully: Do we need to do anything at all, what makes sense, what do we no longer need to do?
Compensatory increased prostate secretion is produced, with reduced sperm. After the conflict has been resolved, which may consist, for example, in the patient regaining his young girlfriend or compensating for the loss with a new, young girlfriend, the ejaculate is restored to its former level because only the former amount of ejaculate is needed again. The additionally formed cells (so-called prostate tumor = prostate hypertrophy = prostate enlargement) have become superfluous and can now be broken down again tuberculously.
Copyright Dr. Hamer
Translated: John Holledauer