
If one found glia accumulations in the brain in the brain-computer-tomogram, since this existed, which were also well stainable with contrast medium, then the diagnosis was usually certain: brain tumor!
In 1982 – one year after discovering the IRON RULE OF CANCER – I succeeded in prospectively finding a Hamer Focus point of considerable dimensions in a patient with territorial conflict in the healing phase and a myocardial infarction happening in the epileptoid crisis. From then on, I knew that there were no brain tumors but that these phenomena must all be related to the healing phase of a biological conflict event.
The Hamer Focus – the expression originates from my opponents, who disparagingly called these formations found by me in the brain “the weird Hamer Focus.” This Hamer Focus I now observed closely and was soon able to recognize such, whose supposed formation I could follow from the beginning of the healing phase.
However, since I had already very quickly found the law of the two-phase nature of diseases, I naturally knew that a conflict-active process also belongs to each such healing phase process.
The misfortune for many patients wanted it that the Hamer Focus is repaired in the healing phase by storage of glia cells (connective tissue). This is accompanied by the tissue’s increased rigidity but remains without discomfort as long as the organism does not get sick again from a conflict in the same place.
Enormous difficulties arose:
1. in the case of cancer – and of course, I concentrated on this disease at that time because I thought I had only discovered the mechanisms of the development of cancer. It was not usual at that time to make a CT of the brain unless there were justified reasons to assume brain metastases. It was therefore challenging in individual cases to have such a CT of the brain made at all. Since computed tomograms were disproportionately expensive at that time, one was happy if one could get a single series of computed tomogram of the brain at all.
2. I started compiling Hamer Focus’s topography in the brain, which was very difficult. Because if something was seen in the brain, it could also be an old process that had already run its course and no longer had anything to do with the patient’s current conflict events. Besides, I did not know whether the patient had other carcinomas that had just not been diagnosed yet, which was also possible with new processes or very current biological conflicts.
3. I found overlapping conflicts with similar conflict content that I now know had covered multiple relays with a single Hamer Focus. I.e., the patient had suffered a conflict or several that had different conflict aspects that had all hit the patient at the same second of the DHS and were all combined into one large Hamer Focus.
4. some patients had several HHe at the same time at entirely different areas of the brain. However, all these foci had one thing in common, they had to represent the healing phase if the patient otherwise showed all symptoms of the conflict-resolved pcl-phase.
5. To all these HHs in the healing phase, there had to be some formation in the brain, which one would have to make visible with some apparatus, which would correspond to this conflict in the active phase. There I sometimes saw such target-shaped circles, which were always mildly smilingly dismissed by the radiologists as round artifacts of the apparatus. There were also semicircular structures, both those bounded by the falx and those that appeared to be bounded by the CT’s lateral image edge.
6. The cooperation of radiologists was practically zero. A number of them had radiation equipment and did so-called X-ray radiation therapy. And such former colleagues could not afford to even think my results were possible. The rest told me quite bluntly that not very many radiologists had a CT machine – that from the moment they considered Hamer’s theories possible, they would not get a single order from the clinics. If a brain CT was performed, it was usually only to find a brain tumor or “brain metastases.
7. Since I did not have my own CT scanner, I did not have the opportunity to perform systematic examinations or repeat the examinations with a different cutting angle. We could only get “what fell from our masters’ tables,” and that was not much. It often happened that the computer tomograms were not given to the patients. With the written findings, however, one could do almost nothing.
8. I knew and knew the Hamer Focus or the ones that I thought belonged to the healing phase. I postulated that these HH must have existed already in the conflict-active phase, but the radiologists did not accept this: “Mr. Hamer, we see nothing there.”
9. I saw many Hamer Focus, but I could not imagine cancer, e.g., the motor, sensory and periost-sensory relays in the brain, which did not make cancer on the organ level, but at most represent a cancer equivalent. However, I had not expected these diseases but only cancer. And that’s why it often happened to me that I had much more HH than I was actually looking for, and in the cases where the patient had only a conflict activity and not yet a solution of his conflict, there was nothing found.
It often happened that the patient had a massive tumor, and they found “nothing” in the CT scan of the brain. Others had a small tumor in the healing phase, and an extensive Hamer Focus was found in the brain.
I had no choice but to follow every natural scientist’s path. As a good craftsman with 99% perspiration and 1% inspiration, to compare all computer tomograms of the brain that were at all possible, together with the corresponding or supposedly corresponding organ findings, with another brain CTs, which in turn had other organ findings.
In the beginning, another difficulty was that I could not distinguish between left- and right-handedness, so, as I know in retrospect, I would have been in error even more often if I had not always started from the organ. The correlation is always evident from the organ to the brain or from the brain to the organ. Only with the correlation between psyche and brain or brain and psyche, the left- and right-handedness is essential.
So an example: Either a right-handed woman gets hemorrhoids during an identity conflict in the healing phase, or a left-handed man gets hemorrhoids during a territorial anger, also in the healing phase. However, suppose I see a Hamer Focus with edema at a specific location on the left cerebral side in the left temporal lobe. In that case, the patient must always have a hemorrhoidal, i.e., rectal squamous ulcer in the healing phase. Conversely, if the patient has rectal ulcers in the healing phase, i.e., hemorrhoids, he always has a HH in the brain at the left temporal lobe in the healing phase.
I succeeded first based on many hundreds, later many thousands of computer tomograms of the brain, finally to learn to distinguish between cancers and cancer equivalents, then to be able to determine the correct localization or correlative topography to the organ. It must be emphasized that for many bodily functions, such as periosteal sensitivity, which indeed covers our entire skeletal system, there was only a white spot on the map of the brain and on the map of the organs because this periosteum could be studied so poorly or not at all. Periosteal sensitivity is not reported in any textbook.
There remained controversy about the so-called ring artifacts, which exist but are seen only once in every 100th patient and are regarded by me as Hamer Focus in target configuration, i.e., the conflict-active phase. The alleged ring artifacts denied by me, with few quite clear exceptions, quite vehemently, or are just claimed as HHe in shooting target configuration, are always denied by the radiologists as facts and just considered artifacts, i.e., art products of the apparatus.
For years, attempts were made to simply push these phenomena aside. Finally, a good idea came to me, whereby my 12-semester physics study came in handy. I contacted the head of the Siemens manufacturing company’s computer tomography department, Mr. Feindor, with a “request.” We had a pleasant discussion in which I asked him that the two of us would like to determine which criteria would have to be fulfilled in the case of ring artifact and when there could certainly be no ring artifact. Mr. Feindor is an engineer, and we had no problems at all in determining the conditions which should be fulfilled or not fulfilled in this or that case. That was on 18.12.89.
On 22.12.89, the final protocol was signed. Since then, real panic has broken out among neuroradiologists. We felt this immediately when we planned a test series at Siemens in the new year 1990. I asked Director Feindor to allow me to carry out a series of tests at the Siemens factory in Erlangen, which was to last about four weeks. After that, many neuroradiologists were invited, who were then to confirm with Siemens that the cases presented could not be artifacts but represented objective findings, i.e., facts.
The date for this scheduled conference was now delayed continuously until one day, a responsible person of Siemens told me in confidence: “Mr. Hamer, we have got the very worst trouble with the radiologists.” Clear disapproval had been signaled…
In preparation for this conference, we had done all kinds of examinations originally agreed with Siemens. Such as moving the patient 2 cm to the left from the center position during the CT examination or then moving him another 2 cm to the right to see whether the shooting target configuration always remained in the same place in the brain, which it did. Or we tried to make progress checks on the same patient at as regular intervals as possible, if possible on different apparatuses, to see what course the shooting target configuration took.
It was also a sure criterion for a genuine finding if the shooting disc configuration occurred only in a certain number of slices, but no longer in other slices.
During all these examinations, which took a lot of time and effort and a lot of right coaxing from the radiologists, we found one quite astonishing thing: A radiologist once said that he also saw these shooting targets on organs. They must really be artifacts there.
From that moment on, my bright interest in such organ shooting target configurations was aroused, and I studied them systematically. I found that there really were shooting target configurations in the compact organs on which we can do CTs, such as the liver, spleen, renal parenchyma, bone, etc. Still, they were usually visible only initially, possibly becoming visible again in the bone later when the bone recalcified. It resulted in the astonishing fact that the brain and the organ corresponding to each other in shooting target configuration, and these shooting targets also have an individual course at the organ. For example, in the liver, we see the classic shooting target configuration only at the beginning in solitary liver Ca. Later, the solitary liver Ca becomes dark in tomography and no longer reveals a shooting disc configuration. In the case of natural healing by tuberculosis, we can undoubtedly see indicated calcareous rings, especially if a whole cavern. I.e., a hole in the liver had not occurred, but if the hepatic Ca had stopped halfway and in the case of natural tuberculous healing, the solitary round focus only had to be thinned out.
If you look at the whole thing correctly, then we have, on the one hand, the head brain that we are all familiar with. On the other hand, there are the organ cells, each of which has a cell nucleus. Organ cells are networked with each other, and each cell nucleus, i.e., mini-brain, is also networked with all mini-brains of the body.
We can regard the sum of these mini-brains as a second brain. This would then mean that in the event of a biological conflict, one area of the head-brain, which we call Hamer Focus, would correspond with another area of the organ-brain, which we previously called cancer or cancer equivalent or organ alteration.
In the case of a sensory stimulus, for example, the organ brain supplies information to the head brain; the other way around, the head brain supplies information and commands to the organ brain in the case of a motor response.
We do not yet know precisely what is happening electrophysiologically in the brain’s individual cells and organs or in overlapping areas or relays. Still, this knowledge is not a prerequisite for our clinical work with these clear findings.
In DHS, the responsible relay center in the brain is marked, and a so-called shooting target configuration marks it. Around the center of this relay, sharp circles, we also say concentric circles, are formed, which look like shooting targets. “Shooting target” means the Hamer Focus is in the conflict-active phase.
In this case, the location does not arise by chance, but it is the computer relay that the individual “associates” with according to the conflict content in the second of the DHS. In turn, from this Hamer Focus, in the very same second of the DHS, the organ of cancer correlating with the Hamer Focus is affected. Surprisingly, we can also prove the organ’s affectedness by a shooting target configuration in the organs that we can tomograph in CT as compact organs, such as the liver, spleen, bones, kidney, etc.
As the conflict progresses, Hamer Focus in the brain also progresses, i.e., a more and more extensive area is affected, or the once affected area is more intensively altered. At the same time, cancer in the organ also progresses. I.e., the tumor becomes larger in mass (so in the inner germ layer), more extensive in necrosis (so in the middle germ layer), ulcerous larger, more extensive, by many small ulcers (so in the outer germ layer) due to true cell mitosis.
In my first paperback from 1984: “Cancer – a disease of the soul, a short circuit in the brain…” I had still called this Hamer Focus in the conflict-active phase a short circuit because we knew nothing about the bioelectrical processes. Today I don’t call it so anymore because, by a short circuit, we generally understand a disturbance of the program. But that is only conditionally the case with the Hamer Focus. We can say it is a disturbance of the everyday program, with which the organism, however, already expects that it could occur one day:
But the word “disturbance” is inappropriate because it is a kind of emergency or special program. I.e., suppose the individual is unexpectedly “caught on the wrong foot” in a situation it had not expected. In that case, an emergency program sets in. We call this biological conflict, which aims to bring the individual back into the normal rhythm. This emergency program does not only refer to the individual alone. Still, depending on the case, it includes several or many conspecifics, in that it can also refer to family or clan.
For example, a mother witnesses her three-year-old child having an accident and becoming unconscious before her eyes. If this is a DHS for the mother, it triggers a biological conflict, and a particular one at that, namely a mother/child care conflict. This biological conflict has particular sensible meaning at all 3 levels: all thinking and doing revolve around getting the child well at the psychological level. On a cerebral level, we see in a right-handed woman in the right lateral cerebellum a shooting disk-shaped Hamers’ focal point, which shows us that conflict activity is going on in this mother/child conflict. On the organic level, we see that the woman and mother’s mammary gland tissue is growing. So the left breast increases by a certain amount of mammary gland tissue – this is still common in nature or among primitive peoples – it is involved in milk production so that the mother produces more milk than before. The consequence is again that the child gets more milk and can get well faster. Once the child is healthy again, conflict resolution sets in, i.e., now the excess mammary gland cells are no longer needed because the child can now make do with the usual amount of milk again. The further consequence is that during the breastfeeding process, tuberculosis sets in, so the child practically gets tuberculous milk, which does not harm it at all. Tuberculosis cauterizes the newly grown mammary gland cells and breaks them down. What remains is a cavern.
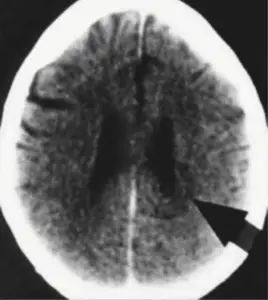
But what are these tumors in the brain, which, when they are clearly visible, i.e., are already in the healing phase? They are called brain tumors or brain metastases by neuroradiologists. If they are less clearly visible, they cause general perplexity. If they show a very strong perifocal edema and Hamer Focus can be easily visualized, they are called rapidly growing brain tumors;, if they show intense perifocal edema, but the Hamer Focus is not visible, as mostly those of the cerebral medulla do, again cause general perplexity; which, if they are located at the cerebral cortex, are misinterpreted as tumors of the meninges. But which are basically always the same, only the different stages of the course of a Hamer Focus!
Hamer Focus in the conflict-active phase, namely the shooting-disc configurations, has always been misinterpreted as artifacts of the apparatus. If they got edema later and became so-called brain tumors, the radiologist usually did not bother to determine that this supposed brain tumor had been visible earlier as a shooting target configuration, i.e., as a Hamer Focus in the conflict-active phase. Since the SIEMENS company and I signed the paper cited at the end of this chapter, the alleged artifacts’ discussion should finally be over. They were facts: I.e., the shooting targets signified the conflict-active phase in a particular relay or relay group of the brain.
Brain tumors do not exist by definition: brain cells cannot divide after birth, not even under conditions misinterpreted as brain tumors. In other words, entirely under no conditions at all. What can proliferate is harmless glia, the brain’s connective tissue, which has precisely the same function as our body’s connective tissue. No one can classify glial cells with any certainty in terms of their developmental history. According to how they behave in the brain, there is an urgent suspicion that they are of mesodermal origin. This is indicated by the fact that the glia is always deposited in the brain relays during the healing phase.
On the other hand, we know that neurofibromas develop or make cell proliferation in the conflict-active phase. But this is not a contradiction because we know that the mesodermal organs include both the cerebellum-controlled organs and the cerebral medulla-controlled organs. The former make cell proliferation in the conflict-active phase, and the latter group makes cell proliferation in the healing phase. We must therefore assume that gliomas have both capabilities of the mesoderm. These bright glia-dense Hamer Focus are repairs of the organism to the Hamer Focus, the reason for joy instead of fright or even brain surgery.
Let’s go through how something like this works in order:
In a DHS, the “responsible relay center” in the brain is marked, and thus Hamer Focus in shooting target formation. As soon as we see this shooting target configuration in a specific relay in the CCT, we know that a special program runs in this relay. I.e., the organism has been caught on the wrong foot in this conflict, brain and organ area, and has switched on a special program.
This special program ensures that the organism copes with the unexpectedly occurred situation, which may affect the patient as an individual and possibly also, for example, his biological group (clan, family, etc.). The conflict activity, i.e., the shooting target configuration in the brain, lasts until the conflict situation is resolved, and the organism can return to normal. However, until it can do that, the organism must pay the price of having initiated the special program with a kind of short-circuit, representing a kind of emergency program. The price is the healing phase, i.e., the repair of the psychic, cerebral, and organic level, to regain the previously optimal state. The organism can return to normality only when this is achieved through the healing phase or the repair on all three levels. As long as the special program in the form of shooting target configuration, i.e., the conflict-active phase, also called permanent symphaticotonia, exists in the Hamer Focus, the brain relay – as we can imagine it – is clearly affected.
We can imagine it as too large an amount of current at too high a voltage being chased through too narrow a line. The line burns out, i.e., of course, the insulation first. In bio-electricity, it is a bit different again, and in the brain, we have to imagine the brain cells arranged like in an infinitely complicated grid. Through permanent sympathicotonia, which is in principle, something planned (just too much of a good thing), now the brain nerves’ communication lines are increasingly damaged. Just as the body organ is enlarged, reduced, or in any case changed by cancer, to accommodate the special new, unexpected situation. Until the end of the conflict-active phase, nothing exciting seems to happen at the Hamer Focus, at least as far as CCT is concerned, except that the shooting target configuration remains constant. For example, in the MRI, we can see that there is a difference from the surrounding area, but it looks completely undramatic.
However, the reality is quite different, and we can estimate the damage only when the conflictolysis has occurred. Now, in the pcl-phase, we can overlook the whole extent of the change or damage. Because precisely with the beginning of the pcl-phase, the organism starts to repair the damage of this special program – be it cell proliferation at the body organ, be it cell reduction at the body organ – and, of course of the affected brain relay.
psychological:
A. Conflict-active phase (ca-phase):
Permanent sympathicotonia, i.e., maximum stress. The patient thinks about his conflict day and night and tries to solve it. He does not sleep anymore, and if he does, then only in the first half of the night, half-hourly, he loses weight, he has no appetite.
B. Conflict-resolved phase (pcl-phase):
Immobilization takes place. The psyche must recover. The patient feels listless and tired but is as if redeemed, good appetite, and the body is hot, often fever, and often a headache. Patients sleep well, but usually not until three o’clock in the morning. This mechanism is set up by nature so that individuals in vagotonia do not sleep until daybreak so that potential danger (e.g., predator) does not surprise them in their sleep. The patients all sleep a lot and very much during the day.
cerebral:
A. Conflict-active phase (ca-phase):
Shooting target configuration in the associated Hamer Focus (see diagnostic chart), i.e., that a special program is running here.
B. Conflict-resolved phase (pcl-phase):
Hamer Focus is repaired with edema formation, and glia is deposited in the affected relay area. This largely restores the previous state, which is essential for later conflicts, but the price is that the tissue is less elastic than before.
organically:
A. Conflict-active phase (ca-phase):
According to the diagnostic chart and the scheme of the ontogenetic system of tumors and cancer equivalents, either a cell proliferation, which has a definite sense of biologically, or cell necrosis. I.e., cell shrinkage or a hole, which also has a particular sense biologically, occurs in the conflict-active phase. The sense is that this extraordinary surprise situation, which we call the biological conflict, can be solved with the help of the organic change that is made. According to the biological sense, for example, a coronary ulcer ensures that the coronary arteries are dilated in the conflict-active phase. More blood can flow through the coronary arteries, and the individual’s strength and endurance increase. An increase of the mammary gland cells, for example, offers more milk to the child to accelerate the recovery of the injured child.
B. Conflict-resolved phase (pcl-phase):
The repair of the cancerous tumor by microbial degradation or cancerous necrosis by microbial construction is started (see chart and scheme of the ontogenetic system of tumors and cancer equivalents). Always we find both in brain and organ edema as a sign of healing.
Copyright Dr. Hamer
Translated: John Holledauer




