
Germanische Heilkunde® is a coherent set of biological laws that embrace the relationship between psyche, brain, and organs. It also outlines the embryological-ontogenetic explanations in order to understand why the individual relay centres are located in the different locations in the brain. It is always possible to find the brain localisation of each biological conflict in the region of our brain that was “under construction” at the time when this new behaviour pattern was programmed.
For example, when “mother/child behaviour” was programmed into us mammals, it was just the cerebellum that was “under construction”. When sexual behaviour was programmed into us, the cerebrum was “under construction.” GHK teaches us that with biological conflicts we will find the corresponding Hamer Focus (HH) in the brain at these “under construction” places at the moment of conflict.
This means that each conflict content has a very specific cancer and a precise location in the brain.
Furthermore, every “disease” also has its biological sense. The biological conflict that leads to cancer is always a tremendous conflictive shock that catches a person or animal on the wrong foot, or in mid stride and in GHK we call this a DHS (Dirk Hamer Syndrome).
In GHK we can not only immediately determine the nature of a conflict or the conflict content from the computer tomogram (CT scan), but we can also decipher whether a conflict is in the conflict-active phase or already in the healing phase. Cancer “grows” as long as the conflict-active phase continues, and as soon as the conflict is resolved, the healing phase begins in the brain, and in the corresponding organ. The Iron Rule of Cancer states that all cancers can be traced back to these simple basic formulas. For some, this seems too simple and for others too complicated. But the laws of nature are always both at the same time.
Germanische Heilkunde® is based on 5 biological laws that cover all ‘diseases’.
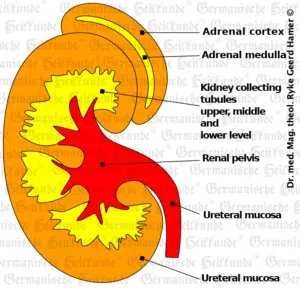
The conflict content in a refugee or existential conflict includes “having lost everything” and “being bombed out.” In the conflict-active phase (ca-phase), a compact tumor forms between the renal calyces and tubules. If we visualize the refugee conflict developmentally, as an ancient archaic conflict, controlled by the brainstem, the biological sense lies in the conflict-active phase. This means that the active water retention. i.e., the emergency brake or the special biological program (of an individual thrown out of the water by misfortune on land) to hold on to the precious water in the organism to prevent the threatening dehydration on land as long as possible. For this purpose, a tumour in the collecting tubes, a renal collecting tube carcinoma, is formed so that the “excretory sieve” becomes virtually clogged or compressed to retain the organism’s water. Hence the oedemas in renal collecting tube carcinoma.
In the healing phase (pcl-phase), renal tuberculosis used to be diagnosed radiographically from the renal pelvises or renal calices. Some of which were very clumped together, i.e., compact adeno-Ca tumors are cauterised by mycobacteria (TBC). The renal calices appeared clumped due to the caverns.
While we used to believe that we had to surgically remove all cell proliferation, i.e., tumours, or at least poison them with chemo, Mother Nature not only has a much more efficient surgical technique with tuberculosis than we could ever develop, but these surgical measures are always applied only in the healing phase. (see: The ontogenetically conditioned system of microbes).
This type of healing was previously called nephrosis or nephrotic syndrome. According to conventional medicine, nephrotic syndrome is a complex clinical symptom. It is considered a consequence of altered permeability of the glomerular basement membrane, both in inflammatory and degenerative kidney diseases.
And since, by its very nature, this conflict often has recurrences and then resolution phases, the nephrotic syndrome was considered chronic.
In Germanische Heilkunde®, it is a healing phase of a renal collecting tubular Ca’s and protein loss by wound secretion in the area of tuberculous caseation. Just as tuberculous caseation of a breast tumour produces a lot of wound secretion in the pcl-phase, the same wound secretion is produced in the renal pelvis during the caseation of a collecting tubular carcinoma. The therapy consists of substituting the hypoproteinemia (lowered serum protein level) with albumin infusions until the healing phase has reached its definitive conclusion. The accompanying symptom of profuse sweating (night sweats) is usually of little concern to patients who know about it in advance and are psychologically prepared for it. In contrast, it often causes panic in unprepared patients. Nephrosis or nephrotic syndrome was neither a disease nor a syndrome, although it almost always led to death.
Renal failure (renal insufficiency) is either the conflict-active phase or the hanging healing. The initial tissue (renal collecting tube tissue) melts away in a tuberculous hanging phase.
Differently with the water or liquid conflict (pith)
Here we see in the conflict-active phase renal parenchyma necrosis, i.e., necrosis of the renal tissue and increased urinary substances (creatinine, urea). At the same time, blood pressure is always elevated in this phase. Its purpose is functionally to compensate for the hole in the necrosis’s kidney tissue so that sufficient urine and urea can be excreted. This means that the blood pressure is also elevated as long as the conflict is still active.
We know that not pre-kidney or primordial kidney but only post-kidney developed to today’s kidneys. So, water conflicts could only exist when our biological ancestors “moved out of the water onto the land” (“rose out of the water”). Most water conflicts have a very tangible reason for the DHS, e.g., a flood, a “near-drowning,” an IV in the hospital, burst water pipes, or the like. In most cases, the problem and its consequences become irrelevant after a few months, and the conflict is usually resolved.
In the healing phase, a protrusion forms from the kidney’s necrosis, filled with fluid. This is called a renal cyst. Inside the cyst, an intense cell proliferation takes place at the end of which – after nine months – instead of the fluid, a solid cell tissue is built with its blood vessel system. During this time, the cyst is “attached” to the surrounding area, but later, it detaches when it is indurated (solidified). In conventional medicine, we used to misinterpret this as “invasive tumor growth” and pseudo-treated it accordingly in a nonsensical way – instead of merely waiting calmly until the attachments spontaneously detach all by themselves and give way to a beautifully smooth, about 1 cm thick, rough capsule of the now indurated cyst. This so-called indurated renal cyst, which is called a “nephroblastoma,” is then part of the kidney and produces urine.
This means that the kidney can now perform even more than before. The biological meaning here is at the end of the healing phase because the kidney can perform more than before due to the forming cyst, which indurates and produces urine. The blood pressure is normalized at the end of the healing phase.
In the first 5-6 months, when the cyst is still partially liquid and already partially solid, it was previously called a “Wilms tumour,” This was always surgically removed along with with the kidney. It is delusional to believe that “malignancy” is responsible for this. One must simply wait nine months. If the indurated cyst is so large that it interferes mechanically, it can be removed afterward without removing the entire kidney.
We used to call the healing phase of the renal parenchymal necrosis or the forming renal cysts, the healing phase of the fluid conflict, glomerulonephritis. We used to fight them as well. However, since Germanische Heilkunde®, we know that at the end of this healing phase, an indurated renal cyst has been formed, which in the further course produces urine and integrates itself into the kidney function.
The fact that the renal parenchyma, diminished by the necrosis, is now replenished, even more than before, makes hypertension’s necessity (high blood pressure) unnecessary for the organism. The renal cyst is never the cause of hypertension, but it was once in its previous conflict-active phase. Hypertension is always the sign of a water conflict, what we have already known in school medicine occasionally as the so-called requirement hypertension. Likewise, the creatinine value rises. However, when the conflict is resolved, the blood pressure immediately drops, and the creatinine value also decreases. If, on the other hand, one tries to lower the required high pressure with medication during the conflict-active phase, then the creatinine value rises all the more!
Until now, however, it was considered that this accounted for only about 5% of hypertension cases. While in reality, except for the cases of Goldblatt-mechanism in renal artery stenosis or the cardio- or aortogenic hypertension, the renal or adrenal ones are, in my opinion, the usual ones, which we just could not recognize until now. Because even the so-called labile hypertension or persistent hypertension were not qualitatively different types of hypertension but differed because some water conflicts again find temporary solutions (then called labile H.), other water conflicts, on the contrary, remained conflict-active (then called constant H.).
In adrenocortical necrosis (cerebral medulla), we have a conflict of “having gone in the wrong direction,” of “being on the wrong track.”
In the conflict-active phase, cortisone production is reduced by necrosis, and therefore, despite sympathicotonia, the run is stopped in the wrong direction (stressed fatigue, Waterhaus Friderichsen syndrome). Also, in this case, increased blood pressure.
In the healing phase, there is now a refilling of the necrosis with cyst formation, and simultaneous enlargement of the NNR volume, and accompanying strongly increased cortisol formation, thus enabling a quick run (e.g., behind the foci) in the right direction (hirsutism, Cushing’s syndrome). Blood pressure returns to normal at the end of the pcl-phase (indurated cyst).
The renal pelvic ulcers (cerebrum) are based on a conflict, which exists in female and male form, e.g. (female) “not being able to mark the territory from the inside” (similar to an identity conflict), e.g. not knowing which opinion to follow, or just (male) “not being able to mark the territory border” (territory marking conflict), depending on handedness. (Clapping test: If the right hand is on top, one is right-handed, left hand on top, left-handed).
In the conflict-active phase, ulcers form in the renal pelvis or calyces, accompanied by spasms and mild pain. If a calyx neck is affected, congestion occurs in the renal calyx, and a renal stone forms.
In the pcl-phase, the ulcers in the renal pelvis heal with renal pelvic inflammation. Likewise, the ulcers in the calyces heal, the spasm resolves, and the patient now has renal colic. The calyx stone, which had formed in the ca-phase, is pushed through the calyx neck, released after the spasm is resolved, enters the renal pelvis, and goes from there through the ureter into the bladder. This process is called renal colic.
Embryology, or the history of human development, is the mother of all medical science. Only it could tell us the secrets of cancer and, thus, of all so-called diseases / special programs because our biological conflicts concern behavioral programs that have been programmed and rehearsed for many millions of years.
Copyright Dr. Hamer
Translated: John Holledauer




