
Bone Ca in Germanische Heilkunde
Initially, cancer was understood to be a tumor with strong cell proliferation. It was assumed that the cells of the tumor could float away and create baby tumors in other parts of the body, what conventional medicine calls “metastases,” which in reality do not exist. When we look at the so-called “bone metastases,” where there is the opposite of cell proliferation, i.e., holes in the bone, it is very clear that no one really knew what “cancer” actually was before 1981.
In 1981 Dr Hamer discovered the IRON RULE OF CANCER, also known as the 1st biological law of nature that outlined his cancer origin theories. But nobody thought that cancer could be caused by a dramatic, highly acute, isolative conflict, which catches us on the wrong foot (off-guard), so to speak.
The DHS (the biological conflict shock) is indeed an experience that catches us off-guard or we are “caught on the wrong foot,” however, there is the opportunity to compensate for this breakdown. Because a “sensible biological special program” (SBS) is initiated at the same moment as the DHS and this is mother nature’s way of setting things back into place.
This biological conflict determines at the moment of the DHS both the localization of the SBS in the brain as the so-called “Hamer Focus” (HH) and the localization of the organ as cancer or cancer equivalent (cancer-like disease, i.e., cell reduction or loss of function). Each disease has two phases: a conflict-active phase and a healing phase when the conflict is resolved.
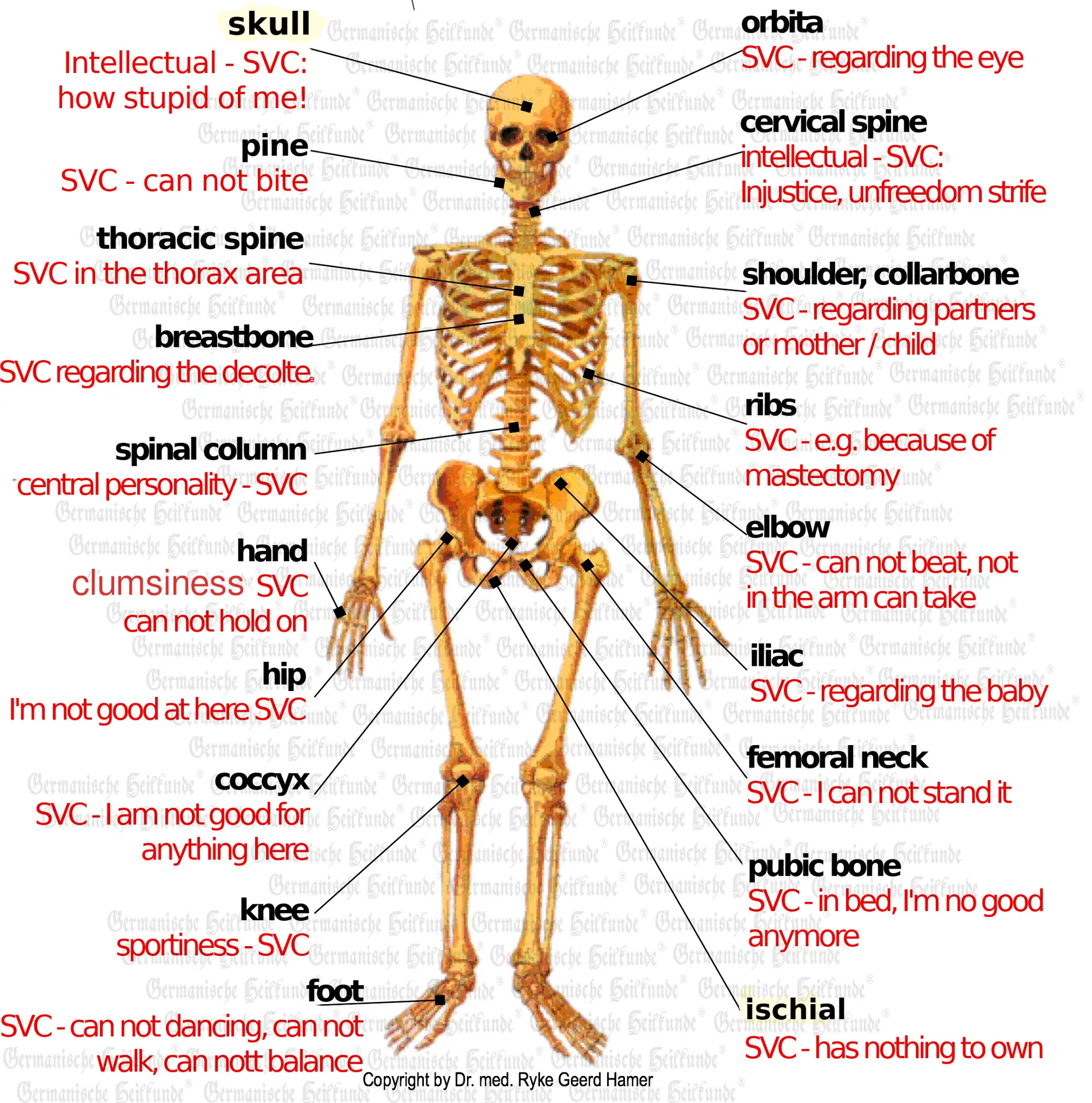
The conflict content in the “bone cancer” is always a conflict of loss of self-value, a self-devaluation conflict (SDC), which can be felt in different ways. How, where, what one feels is always decided in the second of the DHS, e.g.:
Intellectual-moral = calotte and cervical osteolysis.
Concerning mother/child, father/child, husband/wife, and vice versa (depending on handedness) = osteolysis of the shoulder
SDC of manual skills and dexterity = arm bone osteolysis, hands
Central SDC of personality = lumbar and thoracic osteolysis SDC of athleticism = leg bone osteolysis, knees.
In the conflict-active phase, necroses, i.e., osteolysis of the skeletal system, occur. Bone cells are degraded or, in lighter cases, of the lymphatic system, accompanied by simultaneous depression of hematopoiesis and white and red blood, i.e., a reduction of hematopoiesis = anemia.
When SDC conflicts last for a long time, large osteolysis can occur in the skeletal system, so there is then a risk of spontaneous fractures in this conflict-active phase.
After conflict resolution (CL) of the SDC, the exact opposite occurs. A wild but very well-organized proliferation of callus cells sets in. In this phase, however, the bone is initially still in maximum danger of sintering together as long as not enough callus has been incorporated. The osteolysis always recalcify with intense swelling of the bone tissue and severe pain due to tension of the periosteum (bone skin). Simultaneously, a deep dark coloration (edema in the cerebrum’s cerebral medulla) corresponding to the associated skeletal part is now seen in the HH of the brain, but this recedes with increasing re-calcification.
The better the patient prepares for this expected “bone healing pain,” the easier it is for him to endure it. The pain only becomes unbearable when the patient panics. This pain regularly occurs when the bone edemas are in the healing phase. It is a good sign and an essential process in biological bone healing because this pain forces the individual to keep the affected part of the skeleton still, which would be in danger of fracturing under load or functional stress. Usually, the patient would have to lie in bed and not load the vertebral body. Healing can be observed very well by X-ray examination of the bone, namely by progressive re-calcification. The histologists then say that they can no longer see anything because of the calcification. So, there is more bone tissue there than before (hole) and more than in the surrounding area, i.e., more density.
These compacted round areas, bright white on the X-ray, which had previously been bone holes, were now called “osteoblastic metastases” (bone-forming). The bone holes were called “osteoclastic metastases” (bone-destroying). How can these necroses emit “malignant cancer cells” when there are not found in the cell loss. How can “benign” bone osteolysis become a very “malignant” osteosarcoma? The “osteoblastic metastasis” is nothing other than the healing of the bone hole, basically exactly the same as osteosarcoma.
Osteosarcoma was only called osteoblastic metastasis when the periosteum was opened. e.g., to take a so-called “tissue sample.” In this case, the pressurized callus fluid, which had formed in a bone hole for the purpose of healing and had created tissue pressure and bulged the periosteum in the bone, made its way through the opened periosteum into the surrounding tissue, enlarged and hardened the tissue through the callus cells and caused a so-called sarcoma there, a “half-bone,” which was called osteosarcoma. The surrounding tissue would have been “merely” swollen externally if a trial excision had not been made. However, the fluid leaks through the periosteum (diffuses through the periosteum), and the callus cells do not.
According to the understanding of Germanische Heilkunde®, the same histological formation is always found at the same organ site. Even in the case of cancer, test punctures and test excisions are almost entirely unnecessary. According to our experience, we know that the computer tomogram of the brain (CT) can give more reliable information about a histological formation than a test excision.
There is the same process as, for example, in acute-joint-rheumatism, e.g., in the knee, which is the healing phase after a unsportingness conflict and which spontaneously recurs after a particular time. However, due to the severe swelling and the joint’s actually passive deformation, there may be a recurrence of unsportsmanlike conflict because the patient is now even more unable to walk. Such vicious circles are caused either by not understanding or by a real disability in the healing phase.
Such a vicious circle is, e.g., also the primary chronic PCP = polyarthritis, which is based on the following mechanism: The patient suffers an SDC of clumsiness for his fingers or hand skeleton area. Suppose he resolves this conflict, and the periosteum swells. Since it is often osteolysis near the joints, edema pushes in the direction of the least resistance, i.e., into the fingers’ joint or the wrist. Because of the swelling, the patient feels even more awkward than he already felt. And he now suffers a recurrence in the conflict that has, after all, been resolved in the meantime. The recurrence causes the joints’ swelling to go down. But not because they are healed, but because in the renewed ca-phase, they make new osteolysis instead of re-calcification, i.e., the process is reversed. If the swelling goes down again, the patient feels more skillful with his hands and can solve this conflict again. However, the solution causes swelling of the finger joints again. This process goes on and on in waves and can last for many years until there is a deformation of the hands, which again cements permanent clumsiness.
Patients who were previously diagnosed with acute rheumatoid arthritis, e.g., of the knee, now end up in oncology and are treated for osteosarcoma. The mortality of osteosarcoma of the knee is very, very high. We just hadn’t understood that the two are the same until now because we couldn’t understand the difference between a fracture and biologic-conflict-related osteolysis of the bone in the healing phase. The difference between osteolysis caused by a biological SDC conflict and a typical fracture that occurred without such an SDC conflict is that callus formation occurs without much edema formation in fracture. However, the bone after completion of the healing of an SDC is more calcareous and stronger than before. This is also the biological sense.
Previously, if a patient was diagnosed as “malignant,” the doctor was allowed to give him morphine at the slightest sign of pain. The side effects of morphine, such as addiction, respiratory suppression, intestinal paralysis, etc., were taken lightly.
Since pain is something subjective, each time the effect of morphine wears off, patients feel the pain many times more than if they had not taken morphine in the first place. As is well known, morphine doses must therefore be increased continuously. Therefore, the administration of morphine has always been a one-way street, a killing in installments. With Germanische Heilkunde®, we can now differentiate exactly to which phase of the disease the pain belongs, its quality, how long it will last approximately, etc.
It is essential that the patient understands that bone pain is good. It is a sure sign of healing! Cytostatic, on the other hand, prevent healing. In the case of cancers controlled by the cerebrum, a purely symptomatic false success can be achieved in the healing phase since one can immediately block any healing process with cytostatic (chemo). In principle, one can make every boil, every abscess, and even every bee sting decongest with cytostatic. Still, one always only prevents the healing and, consequently, the necessary work of the responsible microbes.
According to the Ontogenetic System of Microbes, we see that microbes fit into the biological process of SBS in a meaningful and developmentally understandable way. They have grown with us and for us, as it were. They are each a member of a control loop of nature, which we had not known. Therefore, in blind zeal, we tried to destroy these useful little helpers with some so-called antibiotics or sulfonamides. Thus, bacteria partly work on the middle germinal sheet’s cerebellum-controlled organs, where they break down cells, and the cerebral medulla-controlled necroses of the organs of the middle germinal sheet help cells build up, e.g., bones. Surgeons have been taking advantage of this knowledge for 50 years. For example, by opening and keeping open a comminuted fracture by perforating it with a series of so-called nails that remain in place because an open fracture that is accessible to bacteria heals much faster than if it were to remain closed. The bacteria promote build-up but also break down protruding or superfluous bone fragments.
We do not die from microbes, but at best, from massive edema in our brains during the healing phase if the conflict had lasted too long. But there is something more.
When bone marrow stem cells are under hematopoiesis depression for too long during the ca-phase due to sympathicotonia, they eventually produce few or no blood cells, e.g., during very long courses of conflict. We call this panmyelophtisis. However, the brakes are rereleased at the beginning of the healing phase. And with a strong push, the bone marrow begins to produce again. At first, many leukocytes (some of them blasts) are produced, most of them unusable. After the usual erythropoiesis delay of 4-6 weeks, erythrocytes and thrombocytes start again in the same way. Again, initially, there are many inferior quality cells, e.g., erythrocytes with reduced oxygen uptake capacity. This results in “delayed anemia with simultaneous leukemia.”
Leukemia is practically a kind of sarcoma-like proliferation of blood cells. After a few days, the organism already discards the only difference: the excessively and qualitatively poorly formed blood cells. The difference between acute and chronic leukemia can only be understood if the specific conflict situation is considered. Acute leukemia results from an acute dramatic self-esteem conflict, usually a one-time thing. In contrast, chronic leukemia results from conflicts that are temporarily not an issue but then break out again and again from time to time.
It is therefore important to know that there is no leukemia without prior active bone cancer.
But even the devastating diagnosis of “leukemia” has to shatter with thunder the self-value that has just recovered and is often the cause of recurrences or new conflict shocks, i.e., so-called metastases. In this leukemic healing phase, the patient is like a tender plant that should not be exposed to the rough air of self-value competition.
Bone cancer, anemia, leukemia, osteolysis, sarcoma, bone pain, lumbago, scoliosis, herniated disc, rheumatoid arthritis, Plasmocytoma, arthrosis, ankylosing spondylitis, polyarthritis, Hodgkin’s disease, etc., are in principle the same, only in different phases of progression or conditions.
Copyright Dr. Hamer
Translated: John Holledauer




