
Brain tumors do not exist by definition
Cancer disease is a disease of our psyche as well as of our brain as well as of our body. It always proceeds according to the IRON RULE OF CANCER, which states that every cancer disease begins with a DHS (Dirk Hamer Syndrome), with a very severe, highly acute dramatic, and isolative conflict experience shock caught the individual on the wrong foot. Each conflict also has certain content, and this is defined in the second of the DHS. This conflict content arises associative, i.e., through involuntary thought assignment. One thinks that one thinks, in reality, the conflict has already hit in seconds before one starts to think. At the moment of this DHS, a particular program switches on practically synchronously. All processes of the psyche and body are connected by the brain and are coordinated there. The brain is quasi the big computer of our organism. The psyche becomes a programmer, body, and psyche again together with the computer’s success organ.
However, the psyche, brain, and organ are only imagined in three levels to work diagnostically and therapeutically. In reality, they are one unit, which we can only register on all three levels. Because in the second of the DHS, we can already see these changes in the brain, which can be photographed with our computer tomography (CT).
They then look like concentric rings of a shooting target or like the image of a water surface into which one has let a stone plop. Such a relay is called a Hamer Focus (HH). The HH localization shows exactly which kind of biological conflict content must be concerned here!
 Hamer Focus is partly projected into the cerebral medulla, but it belongs to the post-sensory cortical center; painful separation conflict concerning the left leg (periosteum).
Hamer Focus is partly projected into the cerebral medulla, but it belongs to the post-sensory cortical center; painful separation conflict concerning the left leg (periosteum).
Source: Summary of New Medicine for presentation in the Habilitation procedure, page 105.
The conflict always corresponds to a particular course of the HH in the brain and a very specific course in the organ. That means: If the conflict becomes more potent, it also becomes stronger at the organ; if the conflict weakens, it also weakens at the other levels; if the conflict resolves, then there is also conflict resolution at all three levels if there is a relapse, i.e., if the conflict comes back, there is again a relapse at all three levels—a fantastic thing to work with diagnostically. One can work reproducibly and logically with it, as in physics. It is an overdetermined system in the strict scientific sense. If you know one level, you can find the other conclusively. This permanent interplay between the psyche, brain, and organ with the brain as the big computer of our whole organism developed over millions of years. We must keep this in mind if we want to understand the following.
From the onset of DHS, the patient has cold extremities, cannot sleep, cannot eat, loses weight, and thinks about his conflict day and night. This phase is the conflict-active stress phase, or also called permanent sympathicotonia. We can think of it as too large an amount of electricity being chased through too narrow a wire at too high a voltage. However, this DHS catches us on the wrong foot, which is an opportunity nature gives us. Because at that moment of DHS, a particular program is turned on. Due to the permanent sympathicotonia, which in principle is something planned (just too much of a good thing), the communication lines of the cerebral nerves are now increasingly damaged, just as the body organ is enlarged, reduced, or in any case changed by cancer, to accommodate the particular new unsuspected situation. Until the end of the conflict-active phase, at least as far as the computer tomogram is concerned, nothing exciting seems to happen at the Hamer Focus, except that the target configuration remains constant.
However, the reality is quite different, and we can only assess the damage when conflict resolution (CL) occurs. Because only in the healing phase (pcl-phase), can we overlook the whole extent of the change or damage. Because precisely at the beginning of the pcl-phase, the organism starts repairing the damage – be it cell proliferation or cell reduction on the body organ – and, of course, also the affected brain relay. And the longer the conflict has lasted, the greater the repairs.
With the beginning of conflict resolution (CL), the organism switches from the stress phase to the rest phase, called vagotonia.
At the psychological level, resting takes place. The psyche has to recover. The patient feels limp and tired but is relieved, good appetite, the body is hot, often fever, and often has headaches. Patients sleep well, but usually not until three o’clock in the morning.
We now see what was previously considered the most important thing at the organ level: cancer stops! Immediately the cancerous tumor’s repair is immediately started by microbial degradation, cancerous necrosis, or microbial build-up.
On the brain level, we see in parallel that the HH now gets edema. The brain’s remarkable resistance to coping with biological conflicts lies in its ability to heal HH again. The brain does this with the help of edema during the healing phase. During the 2nd half of the healing phase – with the onset of the epileptic crisis. During the second half of the healing phase – with the beginning of the epileptic crisis – harmless cerebral connective tissue, so-called glia, is stored in the brain to repair the HH.
If glia accumulations were found in the brain in the brain-computer tomogram, which was also well stainable with iodine contrast medium, then the diagnosis was usually certain: “brain tumor”!
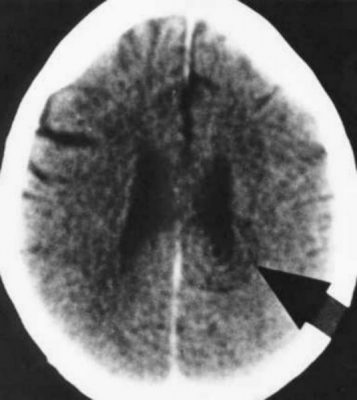
 Hamer Focus (HH) for large resolved territorial anxiety conflict (bronchial-ca) of an elderly patient. In addition, the central conflict in the post sensory cortex center in the ca-phase. The patient’s Sister came to the hospital and told her that she had seen her mother in a dream in a white dress. She said she was going to get the daughter (patient) soon.
Hamer Focus (HH) for large resolved territorial anxiety conflict (bronchial-ca) of an elderly patient. In addition, the central conflict in the post sensory cortex center in the ca-phase. The patient’s Sister came to the hospital and told her that she had seen her mother in a dream in a white dress. She said she was going to get the daughter (patient) soon.
Source: Abstract of New Medicine for presentation in the habilitation procedure, page 107.
However, brain tumors do not exist by definition because brain cells cannot divide after birth, even under conditions misinterpreted as brain tumors until now.
So entirely under no conditions at all. What can multiply is harmless glia – the brain’s connective tissue – which has precisely the same function as our body’s connective tissue. These bright glia-dense HH, which can be seen in the computer tomogram, repairs the organism at the Hamer Focus, thus a reason for joy instead of fright or even brain surgery. However, the MRI technique has the disadvantage of making the organic and cerebral changes appear much more dramatic. This gives the patient the impression that they have a massive “brain tumor,” which appears much less dramatic in the same patient on a CT.
This HH, i.e., a more or less sizeable white spot or area in the CT, then represents the end of healing when it no longer has intra- and perifocal edema. However, the repair price is that the tissue of the HH from then on is regider, not so elastic. The computer brain is repaired in a makeshift way. But there is something else: The patient now has at this psychological conflict scar, as if it were his psychological Achilles heel, his weak point. With this understanding, we can also imagine why a conflict relapse in the early healing phase must have such devastating consequences because the old wound completely tears up again on all three levels. Often the patient still reaches the second healing phase. Still, then the renewed edema shoots in so violently that the brain is over-strained and no longer participates. Now we understand why a re-infarction is usually fatal.
Chemo or radiation now do about visibly what a conflict relapse would do. Healing stops, and the whole swollen relay purrs back together. The edema water is gone, but the HH is not cured with it, not by any means. Thus the catastrophe of the so-called concertina effect has begun. Since the process in and around the HH is not healed but only artificially blocked (stopped), the organism tries after each round of chemotherapy or radiation to restart the healing process immediately, i.e., fill up the HH with edema again. Again and again, the synapses and the nerve cells’ connections are pulled apart. Then they purr together again during the next round of chemo and radiation. The nonsensical game goes on until the synapses tear.
Surgery is even more ignorant. The operation turns the patient into a brain injury victim with all the terrible consequences we still know from soldiers’ brain injuries in war. But not enough with it. The healing of the conflict process is not completed through the operation, but the healing continues as long as it has not been mutilated far into the healthy. The surgical cavity then becomes a cyst, which inflates enormously due to the surrounding edema-producing brain tissue. We do not even want to elaborate on what further interventions, such as drainage, cause.
Hamer Focus with edema or glia always means that a particular program has run in the organism. A conflict resolution must have taken place.
An infinite number of people who were fortunate enough never to have these harmless remnants of cancer, mistaken as brain tumors, carry them around for decades with little or no cerebral disturbance. Except for paralysis (paralysis), most of the cerebral cancer processes are not noticed until the pcl-phase. This is not surprising because only in this stage, they get healing edema and thus become so-called “space-demanding processes.” It is precisely this space-occupying process that has always been misinterpreted as a tumor criterion. Tumor in the original meaning of swelling is indeed, but not in the meaning of carcinoma or so-called “metastasis.” Above all, the HH’s intra- and perifocal edema in the healing phase is only temporary. If we look at the HH after the end of the healing phase, we find nothing left of the space displacement. The spaces between the brain cells are now permanently filled with glia and obviously repaired, which had become defective in (electrical) function by the sympathicotonia during the conflict period. The further particular criterion is that the carcinoma grows in the conflict-active phase and indeed grows by real cell growth, but that the swelling of the HH develops only in the healing phase and only passagerly (temporarily).
Even if in principle, every cerebral edema swells again because it is, like every bodily edema, only of a temporary nature, the patient can die of the cerebral pressure before it has receded again, e.g., in case of a too long duration of conflict or too great intensity of conflict, also a summation of several simultaneous perifocal edemas, unfavorable localizations or also recurrences. Here, for example, a thoughtless word of another person, a doctor, friend, whom the patient considers competent, is often enough to plunge him into the deepest abyss of hopelessness and panic, from which it is difficult for another person, least of all himself, to pull him out again.
Question: Is it possible that all this is really the same in principle: stroke, brain hemorrhage, a brain cyst, brain tumor, meningioma, hyperdense (increased density), and hypodense (decreased density) foci or areas and all the many unclear brain swellings of all kinds?
Answer: With a few exceptions, yes! Of course, falls have relatively rare subdural hematomas (hemorrhages between the dura mater and arachnoid). There are meningitis (inflammation of the soft meninges) and encephalitis, e.g., after injury and surgery. Of course, there are occasional mass hemorrhages in the brain. But apart from these exceptions, which account for no more than 1%, all other brain changes are Hamer Focus, as I said, in different stages of progression, in different localizations, and during or after different durations of conflict. Also, a so-called “cerebral stroke” differs cerebrally from a “heart attack” only because the cerebral process reaches up to the gyrus praecentralis, i.e., up to the motor center under the skull cortical. Thus, the paralysis is in the foreground, which is only temporary, if no new DHS (motor conflict) occurs.
Germanische Heilkunde® is not a sub-discipline that could limit itself only to, e.g., conflict resolution and delegate complications to other sub-disciplines. Still, it is a comprehensive medicine that has to keep in mind all steps of the disease’s course also on the cerebral-organic level. However, medicinal treatment is used in Germanische Heilkunde® to mitigate or avoid complications in the natural course of healing. For example, one would give the patient cortisone if he has too much brain swelling to survive the healing phase.
The DHS is the basis of the Iron Rule of Cancer, and is the linchpin of all diagnostics. With the Iron Rule of Cancer application, the entire medicine and biology order itself as if by itself. In reality, every human being feels and perceives, according to archaic biological control circuits, feels conflicts biologically. At the same time, he imagines thinking he is detached from nature. If up to now we had considered the illness as something hostile, even evil, as a punishment of God, now it appears to us as a sign of a temporary change of nature of our organism, always running synchronously on all three imagined levels, the psyche, the brain, and the organs, which, however, is basically only one organism. Never goes one without the other. Everything always runs synchronously. A downright breathtaking synopsis!
Copyright Dr. Hamer
Translated: John Holledauer




