
The Greeks, with their Asclepius, had developed a culture of coping with psychological conflicts in ancient times. The priests of Asclepius asked those seeking advice about their dreams of the previous night and deduced from them their psychological problems and physical illnesses. Even if, of course, the statements of earlier times could only be global and, for the most part, vague and lacked systematization, one was already closer to the problem of the connection between the psyche and the development of cancer than our 20th century with its fixation on presumed pathological processes and research into facts of the physical level. Also, the unspecific stress research connected with cancer mostly confuses cause and effect, since all cancer patients have stress (permanent stress) in the ca phase. No one could recognize cancer connections since no distinction was made between the conflict-active stress phase with its symptoms and the conflict-relieved vagotonic phase. The psychological “values” are also different for both phases. This led to one examining completely different disease phases and manifestations for a common denominator, which could not exist, out of ignorance of the tumors’ ontogenetic system.
Nor did they distinguish between primary and secondary diseases or even healed, old carcinomas that had only been discovered by chance. Thus, many results of such investigations are meaningless in themselves. Before the discovery of Germanische Heilkunde® in 1981, there were many theories about the origin of cancer. Still, nobody thought that cancer could be caused by a biological conflict, i.e., a dramatic, highly acute isolative conflict experience shock (DHS) that catches us unprepared “on the wrong foot.”
A patient had already lost four very close relatives in a short time but had not suffered a single biological conflict because she had known beforehand with each of these relatives, father, mother, brother, and uncle, that each of the relatives would have no chance to survive. But when the uncle, who had promised to bequeath her a beautiful wooden chest, bequeathed the chest to the patient’s sister in his will, the patient went utterly berserk and suffered a DHS. There she was caught on the wrong foot because she had already firmly counted on it and had even already prepared the place of honor in the living room for it. She suffered an indigestible conflict. After all, she had already appropriated the morsel (chest) in her thoughts and now had to give it out again mentally. She fell ill with pancreatic carcinoma. “Psychologically,” the death (“loss”) of each of these close relatives should have been far more significant – but it was not – because with each of the four relatives, one had known beforehand that here, as sad as it was, nothing more could be done. The relatives were duly mourned, but it had been a psychological or psychological loss conflict, but not a biological conflict. The non-inheritance of the chest hit the patient entirely out of the blue. This caused her a biological conflict and cancer in the pancreas.
But as we will see, pancreatic-Ca is not a “glitch” either, but a sensible biological process. In this context, it is crucial to understand that the same event (e.g., an accident) does not have to cause the same conflict in every person or even cause a DHS. Suffering a conflict is highly individual, and it only decides what the patient himself reports about it.
A. Anger conflict “fight for the morsel,” e.g., inheritance conflicts.
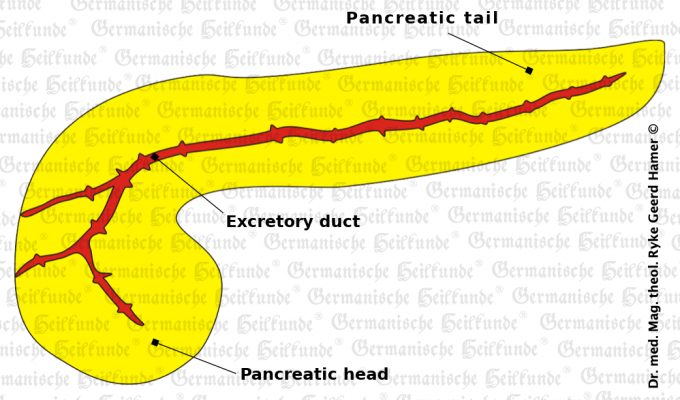
The Hamer Focus is located in the brainstem (pons) laterally on the right side.
In the conflict-active phase, a compact tumor forms. This tumor has the task of producing increased pancreatic juice, which can break down sugar and protein in particular. During this phase, the patient only feels some pressure on the so-called retroperitoneum, i.e., the back peritoneum. Because the pancreas is located retroperitoneal, behind the peritoneum, like the kidneys.
In the healing phase, the patient has the usual TB symptoms with night sweats, etc.
The pancreas is a so-called intestinal appendage organ, like the liver or lungs (alveoli). The pancreas’ biological purpose is to produce more digestive juice to take (digest) the morsel (chest). Or in other words: the increased pancreatic tissue is to be used better to digest the morsel by increased secretion of pancreatic juice.
Even if the morsel is no longer a food morsel for us today, the same applies to the animal – for which the 5 Biological Laws of Nature have to be applied in an analogous way (loss of a morsel) course.
However, most of the cauliflower-like growing pancreatic adenocarcinomas of secretory quality are not as dangerous as they appear.
In the presence of mycobacteria (in DHS): tuberculous caseating, necrotizing degradation with subsequent pancreatic caverns. Most pancreatic adenocarcinomas then do not need surgery because (condition after pancreatic TB:) digestive enzymes can be substituted if necessary.
Cure by encapsulation if no mycobacteria were present at the time of DHS: The patient has virtually no additional symptoms apart from the usual vagotonic symptoms. But he has the “disadvantage” that he now continues to excrete more and more pancreatic juice, although this is biological nonsense.
B. territorial anger or identity conflict – concerning the epithelium (= wallpaper) of the pancreatic ducts depending on handedness, hormonal situation, schizo-constellation, etc.).
Here, the Hamer Focus is located in the cerebrum right temporal.
The pancreas also belongs to the organs, which are functionally assembled from several parts of different germ layers and have different conflict contents.
The pancreatic squamous ulcer, for example, belongs to the outer germ layer and corresponds to territorial anger or identity conflict, depending on the handedness.
In the cerebellum and cerebrum conflicts, handedness is crucial, whereas, in the brainstem, it does not yet play a role. Therefore, the clapping test (applause) is a critical criterion in Germanische Heilkunde®.
If the right hand is on top, one is right-handed, and if vice versa, left-handed.
The Consecutio of the conflicts, i.e., the order in which the conflicts occur, is determined not only by the handedness but also by the current hormonal situation: pill, menopause, hormone intake, removal irradiation of the ovaries, chemo, etc. The left-handed young man, for example, does not suffer a pancreatic ductal squamous ulcer but a rectal ulcer in a territorial conflict. On the other hand, the left-handed young woman in an identity conflict suffers a pancreatic duct ulcer (or gastric ulcer or biliary ulcer).
Typically, a right-handed young woman reacts cortically on the left female hemisphere of the brain in case of an identity conflict. But if the same woman takes, e.g., the pill, she feels male in the conflict and gets her Hamers’ focal point on the right male side.
The correlation is always evident from organ to brain or brain to organ.
Only in the correlation between psyche and brain or vice versa, is the left- and right-handedness essential because it decides about the conflict/brain pathway. Thus, it is also about which “disease” the patients can suffer at all conflicts.
The female identity conflict
Conflict content: “Not knowing where to belong or where to go, also not knowing what decision to make,”
Corresponds organically to a rectal mucosal ulcer in the right-handed person.
Painful rectal ulcers develop in the ca-phase, rarely or not yet bleeding in this phase, but causing pain and spasm and are usually misinterpreted as “hemorrhoid pain.” Again, the biological purpose is ulcerative dilation of the rectum for better defecation and improving location (identity).
In the healing phase, patients have almost no more pain but severe mucosal swelling and bleeding from the healing ulcers. In the past, this severely swollen, ulcerous mucosa, which secretes light-colored blood, was almost always diagnosed as “hemorrhoidal bleeding.” Still, today it is often just as incorrectly misinterpreted as rectal cancer and unfortunately “cured” by surgery with rectal extirpation, which is entirely nonsensical and unnecessary. However, if nothing is done except symptomatic decongestant therapy and conflict recurrences are prevented, then a rectal ulcer heals without problems. However, the same applies here: Caution in the case of simultaneous SYNDROME with carcinoma of the renal collecting duct, a so-called refugee or existential conflict, or conflict of being left alone, conflict of feeling unprovided for or poorly cared for, or fear of hospital, etc.
If in the course of any healing phase in our organism, edema is stored. E.g., in the case of pancreatic ulcer, hepatitis, renal cyst, pleural ulcer or rectal ulcer, etc. Then, if a collecting tube ulcer is added in the active phase, water is stored excessively; i.e., the rectal mucosa can then swell up to double or even more, i.e., cause problems, and likewise, of course, the Hamer Focus in the brain.
Ulcers develop in the pancreatic duct branches and the sizeable pancreatic duct (pancreatic ducts) during the conflict-active phase. The biological purpose is ulcerative dilation of the pancreatic ducts to allow more pancreatic juice to be secreted.
In the healing phase, the ulcers swell the pancreatic ducts; also, serum amylase increases. At this point, the diagnosis of a pancreatic tumor is usually made, but in reality, this is not a tumor but “only” a so-called pseudo-tumor. After swelling has subsided, the affected pancreatic ducts usually become open again.
But also here: Beware of SYNDROME.
Not is rarely this conflict associated with a gastric or biliary ulcer, which also belongs to the outer germ layer, and as a conflict has the same content.
For example, in the case of the stomach-mucous ulcer, it is territorial anger, mainly border dispute conflict, e.g., with the “neighboring territorial chief,” also concerning territorial content. There are regular “stomach types,” which always react with precinct anger.
In the conflict-active phase, there is a loss of substance of the gastric mucosa along the stomach’s small curvature, at the pylorus, and in the bulbous duodena, where the ectodermal squamous epithelium has migrated, which is very sensitive. Hence the pain or gastric colic. The biological sense is the ulcerous enlargement of the gastric passage, especially the gastric outlet.
We often see bleeding gastric ulcers (hematemesis and black feces) in the healing phase. Although this is a good sign, we are used to thinking of it as bad, which in principle it is not. At this stage, the patient has no more pain or colic, except for occasional vomiting.
Intrahepatic and extrahepatic biliary tract ulcer is also a territorial aggression conflict. Boundaries with neighboring territories are violated, allowing the “neighboring boss” to make inroads. Also, often dispute about money.
In the conflict-active phase, ulcers form in the intra- and extrahepatic bile ducts and gallbladder, which hurt. Also, biliary colic or intrahepatic biliary colic. The biological sense here is also ulcerative dilatation in the bile ducts, so the larger diameter improves that bile flow.
In the healing phase, we see hepatitis. This is because the intracanalicular mucosal swelling, to heal the ulcers, causes a temporary bile duct obstruction (icterus) and bile accumulation. Either in the majority of the intra- and extrahepatic bile ducts (icteric hepatitis) or only in a small part (anicteric hepatitis). However, it is not viruses (if they exist) that cause hepatitis, as we clever physicians believe in our simplicity. Still, our organism makes use of them, if they are present and if they exist at all (because they have not been proven yet), to optimize the healing process. If no viruses (if they exist) are present, then the healing phase still runs, of course, but possibly not biologically optimal, e.g., Non-A -, Non-B -, Non-C-Hepatitis.
Our brain always determines which kind of microbes are allowed to help us with which work, and when, and only a certain kind that our brain allows to work there. And likewise, on the command of our brain, the supposedly pathogenic microbes become benign, apathogenic microbes again, which withdraw to some place of our organism, where they do not disturb but where they can be reactivated at any time when they are needed again. The most dreaded thing, both in the gastric ulcer healing process and in hepatitis, is not the gastric bleeding or the elevated liver values (especially gamma-GT, alkaline phosphatase, and possibly bilirubin in the icteric process), but the epileptoid crisis, which occurs just when the liver values begin to fall again.
Extreme caution should be exercised against “hepatic coma” (ammonia formation in the liver), which is cerebral coma, namely immediately after the epileptoid crisis. Therapy consists of continuous glucose administration by os (mouth), and little or no fluid intake with the infusion.
Beware of SYNDROME, which causes hepatomegaly (severe liver swelling) with liver capsule tension pain. Liver values, especially gamma-GT, also rise considerably because of hepatomegaly, which they would do much less without SYNDROME.
But despite all complications, e.g., in long and intensive courses of conflict, which, thank God, are not the rule, most patients manage to get well again. Since we know the Germanische Heilkunde®, we know that pattern cancer develops, progresses, and can also be stopped again – and how we can avoid or end the SYNDROME if possible.
Copyright Dr. Hamer
Translated: John Holledauer




